Numerous causes exist. If you are concerned about your genetic or environmental factors, contact us for a consultation
Anterior Segment Trauma can bring pain and vision loss.
Corneal Reconstruction
In cases of corneal reconstruction after trauma, every effort should be made to conserve a patient’s own cornea when there is the prospect of preserving reasonable functional vision.
The insertion of hard contact lens and performing a check for spectacle requirement over the top, can act as a diagnostic tool of residual functional vision, and provide a measure of potential functional rehabilitation for the affected eye. If hard contact lenses are not tolerated, the use of laser and implant corrections as an alternative to treat any optical disturbance can restore useful vision. If the patient’s own cornea offers no prospect of functional vision, treatment with corneal transplantation may be appropriate.
Iris Reconstruction

Reconstruction with an artificial iris can take many forms. The traumatised iris can be re-sutured to provide an acceptable contour and colour to improve cosmesis.
Artificial iris inserts can be individually painted in an attempt to match the other eye. Other implants are black and simply seek to improve functional vision by reducing glare caused by the aberrant light.
Depending on the trauma to the iris, various styles and shapes for the artificial iris are available to treat most cases.
Iris Base Trauma
The base of the iris is prone to damage during ocular trauma. This can lead to abnormal intra-ocular pressures (either high or low). Both can cause visual loss, and require immediate or delayed intervention to limit damage to the visual potential of the eye.
In most cases, the pressure in the eye is normal but may slowly rise years after the initial trauma. Appropriate follow up for severe injuries needs to be undertaken in those at risk.
Traumatic Cataract
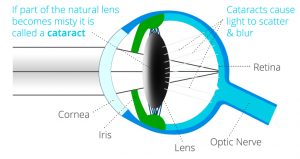
A Cataract is an opacification of the natural lens of the eye. When it impairs the visual pathway, removal is required to improve vision. In cases of traumatic cataract, there is the added concern that the lens capsule could be breached. Leaking lens material into other parts of the eye can cause dangerous intra-ocular pressure rises. Not only that, the lens material itself can induce severe inflammation in the eye. The combination of severe inflammation and high pressure rises can cause irreversible damage long after the initial insult.
Fluid can also leak into the lens through a small capsular rupture. Occult capsule rapture can cause distention and further opacification in an eye that initially looked to have minimal lens damage. This can lead to extension of the lens capsule tear in the eye, and initiate delayed severe inflammation and pressure rise.
Consequently, severe trauma to the eye needs to be monitored closely in the early stages to pick up such events. In rare cases, an isolated peripheral lens breach can be glued using tissue glue which limits cataract formation, and avoids the need for cataract surgery.
Posterior Segment Trauma
Any severe damage to the front of the eye can damage the back of the eye, and therefore the visual potential of the eye. This may be obvious (retinal detachment), but it may also be occult, and vigilance in the initial examination as well as during follow up is required to limit the long term impact of any such injury. Special ultrasound scans help us assess the back of the eye even when no direct view is possible initially.
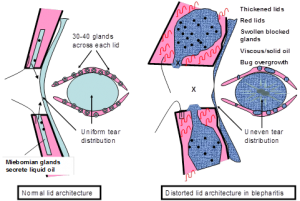 The exact cause of Blepharitis is unknown. One of the main reasons postulated is that the oils, which are normally liquid at body temperature, are turned to a sludge or solid state by an overgrowth of normal bacterial flora which metabolize the oil thickening it up. This then blocks the glands, leading to inadequate amounts and poor quality oil in the tear film.
The exact cause of Blepharitis is unknown. One of the main reasons postulated is that the oils, which are normally liquid at body temperature, are turned to a sludge or solid state by an overgrowth of normal bacterial flora which metabolize the oil thickening it up. This then blocks the glands, leading to inadequate amounts and poor quality oil in the tear film.
These factors induce inflammation on the ocular surface to variable degrees, but not usually causing overt infection. Finally, a viscous circle ensues of increasingly viscous oils in the glands leads to blockage of the glands, chronic dilatation of the glands and loss of normal architecture and function.
Most people will experience repeated episodes of blepharitis and then have long periods of time where they do not have any symptoms. Symptoms tend to be worse in the morning, and both eyes are typically affected.
Symptoms include:
- Itchy, sore red eyelids
- Eyelids stick together, difficulty opening the eyelids on waking due to matting
- Eyelash encrustment
- Burning, gritty sensation in the eyes,
- Increased sensitivity to light (photophobia),
- Abnormal eyelash growth
- Loss of eyelashes
Pre-existing skin conditions such as Rosacea or Seborrhoeic dermatitis
 Developing a regular routine of eyelid hygiene is essential in the long term treatment of Blepharitis. It is important that you clean your eyelids every day, whether or not you are experiencing any symptoms. You should consider it part of your daily routine, like showering or brushing your teeth. Effective eyelid hygiene will reduce both the severity and frequency of symptoms.
Developing a regular routine of eyelid hygiene is essential in the long term treatment of Blepharitis. It is important that you clean your eyelids every day, whether or not you are experiencing any symptoms. You should consider it part of your daily routine, like showering or brushing your teeth. Effective eyelid hygiene will reduce both the severity and frequency of symptoms.
A trilogy of fist hot compresses to the lids, then lid massage and finally a mild detergent lather to the lid margins form the core of this very mundane but effective management. Blepharitis cannot be cured only kept in check with regular lid hygiene if problematic.
In more severe cases, the use of antibiotic ointments or tablets may be recommended if there is no improvement in symptoms after a longer period of regular eye lid hygiene.
A cataract is a clouding of the eye’s natural lens. The lens is normally completely clear.

Normal Clear Lens (left) / Cataractous Lens (right)
However, when a cataract forms, the lens slowly becomes discolored (yellow or white). Because the lens focuses light inside the eye, vision slowly becomes blurry as a cataract forms.
Cataract is the leading cause of blindness throughout the world. While easily treated with surgery, most people affected by cataracts are not aware it can be successfully treated.
Cataracts occur predominantly in people aged 60 or over, as part of the normal ageing process. It can also occur in people as young as 40 due to other risk factors. The development of cataracts is similar to other age-related changes in the human body.
Risk Factors:
Risk factors for development of Cataracts include:
- Older
- Diabetes
- Smoking and alcohol use
- Prolonged exposure to sunlight (U.V light)
- Trauma and previous intraocular surgery
- Long term use of steroid based compounds
Patients with Cataracts can expect common symptoms that include:
- Cloudy or blurry vision.
- Fading of colours
- Glare from light sources (such as headlights, lamps)
- Sunlight may also appear too bright
- Halos may appear around light sources.
- Poor night vision (especially when driving).
- Double vision or multiple images in one eye. (This symptom may clear as the cataract gets larger.)
- Frequent prescription changes in your eyeglasses or contact lenses.
Depending on the visual impairment and progression of the patient’s Cataracts, there are a few choices to improve visual acuity.
Prescription Glasses
Patients with cataracts can update their spectacles at the first instance to avoid surgical intervention. Once the cataract progresses, it will impede the distance visual acuity and the law of diminishing return applies with respect to the benefit of further spectacle updates.
This procedure is the removal of the cloudy lens along with the insertion of an artificial intra-ocular lens to take its place. There are several different types of procedures to remove the cataract. The most commonly utilized technique is Phacoemulsification with Insertion of an Intra-Ocular Lens.
Phacoemulsification and Intra-ocular Lens implant
The purpose of surgery is to replace the cloudy lens with a clear lens implant inside the eye. Phacoemulsification is the procedure where the cloud lens is removed through a small incision (@2mm) in the cornea. The thin clear membrane (capsule) holding the cataract is left intact to support the new lens implant. A thin ultrasound probe is inserted into the eye that uses ultrasonic vibrations to dissolve the lens. These tiny fragmented pieces are then suctioned out using the same probe. Once the cataract is removed, an artificial lens is placed into the same thin capsular bag that the cataract occupied. This intraocular lens is essential to help your eye focus after surgery.
It is unusual to require a stitch in the eye at the end of the operation because the incision is so small it is nearly always self-sealing. Eyes that have a thin corneal wall (keratoconus) tend to be floppy and these do require a stitch to avoid wound sag and degradation of the expected visual outcome.
This procedure requires the use of anaesthetic. Topical anaesthetic drops, such as eye drops and sedation work well. Although eye drop anaesthesia does not numb the eye completely it does provide very effective numbness. Occasional pressure on the eye is all that is likely to be felt at certain points during the operation but sharp pain is very uncommonly reported by most patients. Larger volumes of anaesthetic can be deposited around the eye and can stop the eye moving as well as feeling anything at all (peribulbar or subtenons)
Lens Selection: What sort of vision do you want after the operation?
Depending on an individual’s needs, there are several different intra-ocular lens options available to suit a various ranges of demands. The information below is a brief insight to options available to a patient. Consultation with a specialist Cataract & Refractive surgeon is always required to ensure the patient is suitable for a specific lens type.
Single distance vision (SDV) lens Implants
This utilises a lens with a single focal point, usually set for distance in each eye. It gives good binocular vision over a useful range. If a patient is happy to wear intermediate and reading glasses, then this is the most common option and is usually the only option offered in the public health system.
Monovision
Two different standard lenses (one eye set for distance vision, the other set for intermediate distance vision), then this is a suitable option for those patients who may have had prior experience of it in spectacles or contact lenses. It breaks down stereopsis (3D perception) and you will still need reading glasses for fine print. If you have not tried it before then doing so for the first time at cataract surgery is not the wisest choice. In my practice I reserve this for those who have had experience of this naturally or in contact lenses, for most others tolerance is untested and cataract surgery is not the best place to first try it.
Micro-monovision
One eye is set for distance the other for an intermediate focus point. This is well tolerated as still provides some stereopsis (3D perception) useful range of vision but you will still need readers for all near tasks and occasionally for visual tasks performed at an intermediate distance. This is another very common choice and if the patient is happy to wear readers, you have very happy patient indeed.
Accommodating lens implants
These are lenses that move when implanted in the eye and try to mimic the body’s own natural lens movements. They aim to give good vision over a range of distances. In reality because they move their resting point in the eye is more unpredictable and more people end up a little more short or long sighted than they bargained for. Also most do not move enough and so you still need reading glasses for near and move too slowly so there is a significant lag time ( speed of accommodation ) when you look from the distance to focus on something up close which can be quite frustrating. Others accommodating lenses move too easily in a bid to obtain more near vision and there are a few anecdotes that with a good sneeze one can apparently be left short sighted unexpectedly.
Multifocal Lens Implants
This lens type has both a distance component and reading component. This work in a similar manner to bi-focal prescription glasses except that in glasses the patient looks from the distance into the near add and thus the whole vision sees only one in focus image. With multifocal lens implants both the distance and the near vision are in focus at the same time. When one looks in the distance there is usually nothing obstructing the view at near. When looking at book for near vision, the book blocks the distance image. Multifocal implants offer patients relative spectacle independence and the same operation is offered as a life style choice to patients without cataract who simply want the greater freedom from wearing glasses. They are often referred to as a premium lenses ( a marketing term ) but they truly are more expensive. A period of adaption is required and the compromise with this lens is often noted at night with ghosting, halos and excess stray scattered light. This is most notable when viewing a point source of light at night (e.g. a car headlight).
Not all multifocal implants are the same. Some of the cheaper versions are based on simple prism technology with concentric rings of distance and near which have been around for 25 years and the technology has not changed significantly in that time in my opinion. These diffractive multifocals produce marked halos and light scatter particularly troublesome when night driving. So much so I refuse to offer this particular type of implant as the adaption phase is typically 6-12 months and a significant percentage of individuals remain dissatisfied and less confident with night driving. It also can have a significant explant rate when advocated to the wrong type of patient.
Personally I prefer the segmental multifocal implants. The adaption phase is 4-8 weeks typically and the impact on night driving confidence is consistently reported as much less. Here the near vision is inferior to the distance segment. The aberrations in the vision happens in the vertical meridian (inferiorly) as opposed to the diffractive multifocal implants that produce the 360 degree multiple ring halo effects.


Extended depth of focus and Extended range of vision implants
Here the discussion on optics ranges to the blending of technologies between diffractive IOLS with their course transition and the segmental IOLs with their slow transition from distance to near. Others describe the effect an oil droplet on the lens. A dog with a different tail is my preference. While EDV is the new black on the marketing scene. Reasonably well tolerated….apart that is with the 7% with significant Halos in the FDA trials make this lens like vegemite. You love or you hate it. A potential explant rate approaching in in ten in not my idea of sleeping well. My perception of its relative unpredictability means it has no place in my practice.
Toric lens implants
Patients with high levels of astigmatism can utilise Toric Lens technology, which is designed to counter-act this refractive disorder. Toric lenses correct distortions in one particular meridian/ axis. They can be found in single distance vision lenses and in multifocal implants. Correcting astigmatism is the second most important optical correction, impacting the quality of the unaided visual outcome after correcting defocus, (how long or short sighted a patient is).
Types of eye infections
Conjunctivitis (Pink eye)
Conjunctivitis is an eye infection of the sclera (white of the eye) and it can be caused by bacteria, viruses, chemicals, foreign body or allergies.
Symptoms of conjunctivitis include:
- Eye irritation and redness
- Excessive tearing of the eyes
- A discharge of pus
- Swelling of the eyelids
- Light sensitivity
Patients must follow good personal hygiene such as washing their hands with soap, avoid sharing towels or cloths; along with, avoiding contact with others while discharge is still present. The treating doctor may prescribe antibiotics. Patients should see their doctor as soon as possible to ensure there is no permanent damage from this condition.
Keratitis
Keratitis is inflammation or irritation of the cornea (the clear, domed shape tissue in front of the eye). It can be caused by infections such as; bacteria, viruses, fungi and parasites or it can have non-infectious causes; such as minor injury, dry eyes or other diseases.
Symptoms of Keratitis include:
- Eye pain
- Eye redness
- Excess tears or discharge
- Difficulty opening the eyelids
- Blurred vision
- Decreased vision
- Light sensitivity
- Foreign body sensation
Keratitis can be classified by its location, severity and cause. It can be acute or chronic and examination on the slit lamp is important. Pathology samples may be sent off depending on the clinical presentation. Patients should see their doctor as soon as possible to ensure there is no permanent damage from this condition.
Uveitis
Uveitis is inflammation of the uvea (the middle layer of the eye that consists of the iris, ciliary body and choroid). It can have many causes such as: eye injury, inflammatory diseases; and, exposure to toxic chemicals (pesticides and acids). The type of uveitis you have is classified by where inflammation occurs in the uvea:
- Anterior uveitis is inflammation of the iris (iritis) or the iris and ciliary body.
- Intermediate uveitis is inflammation of the ciliary body.
- Posterior uveitis is inflammation of the choroid.
- Diffuse uveitis (also called panuveitis) is inflammation of all areas of the uvea.
Symptoms of uveitis include:
- Eye redness
- Watery eyes
- Eye pain
- Light sensitivity
- Decreased vision
- Dark, floating spots in field of vision (floaters)
Uveitis can be acute or chronic, but patients should see their doctor as soon as possible as these diseases can lead to reduced vision or visual loss. Treatment is primarily aimed to try an eliminate inflammation, pain and prevent further tissue damage. Plans will vary depending on the type of uveitis and the causes.
 A Pterygium (‘wing of tissue’) is an overgrowth of the conjuctiva that usually only covers the white of the eye onto the cornea. It usually presents in patients over the age of 45, although it has been known to occur during younger years. This is not a cancer as it is a discrete abnormality on the external surface of the eye.
A Pterygium (‘wing of tissue’) is an overgrowth of the conjuctiva that usually only covers the white of the eye onto the cornea. It usually presents in patients over the age of 45, although it has been known to occur during younger years. This is not a cancer as it is a discrete abnormality on the external surface of the eye.
Pterygium can grow at varying rates. They can grow rapidly, slowly, regress spontaneously and restart growing after a long period of time. Occasionally, it may encroach the pupil and enter the line of vision. Pterygium may grow on both eyes but they rarely grow more than once per eye.
Pterygia seem to be particularly common in Queensland. Queenslanders have one of the highest reported rates of occurrence in the world (up to 10%).
- Excessive sunlight exposure in the first 10 years of life.
- Living in a dry and/or dusty environment.
Most patients have no symptoms. Patients do sometimes experience:
- Dry Eyes
- Ocular Irritation
- Cosmetic changes, from the reddish lesion
Decrease in vision (Directly – If covering the line of sight. Indirectly – Changing the shape of the cornea.)
Significant numbers of patients complain of dry eyes and ocular irritation. This can actually predate the onset of the Pterygium. Others are just aware of the cosmetic disfigurement caused by the reddish wing like lesion growing onto the clear part of the front of the eye (the cornea).
Air conditioning, lack of sleep, sunlight, night shifts, and smoke can all aggravate a Pterygium increasing symptoms and redness.
It is important to note that a Pterygium can reduce vision indirectly by deforming the cornea (astigmatism) or directly by covering the direct line of sight through the pupil.
In most cases, no intervention is required. They generally don’t regress and patients should monitor any changes at home. If there are concerns about recent growth, this is a prompt for review by an eye care professional.
In those patients in whom redness is the main issue, the occasional use of an over the counter ‘eye whiteners’ can give temporary relief for important social occasions. Chronic use of these eye drops is not recommended as rebound redness on withdrawing these drops if used chronically.
The use of artificial tears (especially preservative free preparations) can achieve a similar if slower relief of irritation and redness and are often under used, even in eyes without dry eye symptoms.
Surgical excision of Pterygia is indicated for either cosmetic reasons or visual interference. In cases where surgery is undertaken to eradicate symptoms of irritation and dryness, these outcomes are less successful. This is because those symptoms generally predate Pterygium development and they can persist after removal.
The major complication is re-occurrence of the Pterygium. Simple excision re-occurrence rates have been reported as high as 40%. For excision with more advanced techniques, it is between 5 to 15%.
One such modern technique is to combine Pterygium removal with a conjunctival auto-graft along with wide dissection of tenons. The graft is secured with tissue glue from underneath the upper lid area which protects it from U.V sunlight. These all help improve clearance rate to ensure re-occurrence rates are as low as possible.

This pterygium extends to the pupil margin (a+b) however detailed mapping (c) shows a flattening effect of over 8 Dioptres encroaching the central visual axis and far past the pupil depicted as the dotted line. This impacts the vision particularly at night when the pupil is more dilated and more of the pterygium interferes with the enlarged central visual axis. Removal of the pterygium (d+e) removed the troublesome aberrations (f) in the vision and simplified his spectacle prescription.
Pterygium removal utilised a conjunctival graft prepared from non sun damaged conjunctiva under the upper lid. Using a conjunctival graft to cover the defect left after pterygium removal is the gold standard of care currently. The arrows (e) delineate the graft edge. This has been proven to reduce the pterygium recurrence rate from around 40-50% to less than 5%. This pterygium was secured using a tissue glue (d+e) rather than sutures which provides more comfort postoperatively. There is also some weak published evidence to suggest that the tissue glue may also reduce the chance of a recurrence even further compared to using sutures (2%).
Prevention is better than cure.
Things you can do to help reduce your risk of Pterygia include:
- Wearing sunglasses when possible. It is important they are labeled as compliant with Australian Standard (AS 1067.1 1990 Sunglasses and Fashion Spectacles). Also look for an EPF UV rating of either 9 or 10; these lenses transmit minimal UV radiation.
- Children should be kept out of the midday sun. For school children particularly of primary school age, sunglasses should be worn outdoors. Kids of all ages should wear broad-brimmed hats, strollers and baby buggies should have a sun visor and kids wear appropriate sunglasses from the earliest age coaxible.